




























Osteoarthritis of the hip joint (coxarthrosis)- This is a chronic degenerative joint disease that leads to deformation of bone tissue.With cocoin arthrosis, all components of the joint are involved in the pathological process: joint cartilage, bone structures next to cartilage, synovial peel, ligaments, capsule and adjacent muscles.In the case of illness, articular cartilage, micro-redimites of bones and osteophytes (bone growth) are destroyed, and an inflammation of the muscle-ligamentous apparatus in the hip joint occurs.
In the world, every fifth person complains about joint problems with collections.This can be both pain or limitation of movement in the joints and a combination of these symptoms.Every other policinical vision falls on patients with bone muscular disorders, while 66 % of cases are people under 65 years old.According to the latest epidemiological research, the incidence of arthrosis of the knee and hip joint among the adult population is 13 %.
Risk factors for the development of coxarthrosis:
- Genetic disposal.A common cause of the hip joints of the hip joints is the innate or acquired mutation of the type of type II prolagen.
- Older age.The probable cause of the occurrence of arthrosis in old age is a discrepancy between the harmful effect on the articular cartilage that is coherent and its ability to recover.
- Floor.Women suffer more often from osteoarthritis than men.This is due to the effects of the impact of female sex hormones of estrogen on bone mineral metabolism.However, the influence of the floor is ambiguous - according to some authors, unlike damage to other joints, there are no differences in the sexual basis for cox arthritis: In men, arthosis in the hip joint is as often found as in women.
- Excess body weight.The relationship is proven between the excess body mass and the occurrence of arthrosis.Excess adhesive tissue increases the harmful load on cartilage.In addition, adipose tissue produces pro -inflammatory enzymes that damage cartilage tissue.
- Frequent development of bones and joints.In accordance with studies, 80 % of coxarthrosis that occurs without any obvious reason is associated with previously non -diagnosed defects in the development of the hip joint - dysplasia and subluxation.
- Heavy physical work.An excess load on the hip joints with certain types of physical work can lead to damage to the joints and the formation of arthrosis.In danger are agricultural workers, engravers and people with similar work specialties.
- Damage.The risk of developing coxarthrosis increases after an injury to the hip joint.In addition, both a wounded joint and both can be involved in the process.
- Professional plays sports.Professional sports can provoke the occurrence of coxarthrosis both due to the excessive strain on the joints and due to injuries.Potentially dangerous sports include heavy athletics, athletics hopping, parachute sports.
- Bones and joint diseases- Rheumatoid arthritis, psoriasis arthritis, joint infections, avascular necrosis, railing arthritis, etc.
- Endocrine pathologies- Hypothyroidism, hypoparathyroidism, acromegaly (decreased function of the anterior pituitary gland), diabetes, obesity.
If similar symptoms are detected, contact a doctor.Not self -medicine - it's dangerous for your health!
Symptoms of arthrosis in the hip joints
The main symptoms of coxarthrosis include: Pain, Mobility Restrictions and Crunches In The Joints, Your Deformation, Functional Shortening of the lower extremity and periodic swelling of the joints.
Pain at different intensity.The pain in the joint is initially insignificant and occurs for a short time.They appear or intensify as they walk or with other physical exertion, for example during squats, inclinations and weightlifting.As the disease develops, pain intensifies, and even a long rest does not bring relief.In addition, pain with prolonged immobility and fixation of the joint occurs in a position.
Patients complain about the so -called "starting" pain in the hip joints after sleeping, driven in a car and other long -term immobility."Start" pain for coxarthrosis does not last more than 30 minutes.Pain intensifies during hypothermia or in a stressful situation.They can be located in the area with the back or groin on the front or side surface of the thigh.With the spread of pain over the nerves in the lumbar vertebra, it can be transmitted to the thighs away from the center of the body or in the knee.Sometimes the pain applies to the lumbosacral spine and tailbone.

Limitation of common mobility.Movements in the hip joint with cocoin arthritis are limited due to pain.At the same time, rotation (turns both inside and outside) and brings the lower extremity (movement to the center of the body) more often disturbed, but may be limited (movement from the middle axis of the body) as well as flexion and expansion.Inability to make passive movements in the joint due to a pronounced pain syndrome causes a compensatory pelvic bias.The patient's walking changes, the buttocks stick out, the body differs forward when it transmits the weight to the damaged side.With bilateral damage in patients with cocoin arthritis, a "duck is formed".
With coxarthrosis occurs on a regular basisswelling in the jointwhich can be invisible due to muscle and fat layers.The disease is also characteristicThe crystal in the joints during movement, their gradual deformation and functional abbreviation of the lower extremity.
Often a joint is affected by the disease, then the process applies to others.But sometimes arthosis affects multiple joints at once, and polyosostoarthritis occurs.Polyosteoarthrosis is characteristic of the elderly or with a hereditary disposal and contemporary diseases - diseases of bones, joints and endocrine disorders.
Pathogenesis of arthrosis of the hip joints
In the pathogenesis of arthrosis of the hip joints, an important role of mechanically harmful is played (injuries and microtraumas due to increased physical exertion on the joint) and genetic, hormonal and metabolic factors.Often it is not possible to find out which factor has affected the development of the disease in a particular patient, but often the disease develops after tissue damage with mechanical injury.
Damage to the tissue stimulates the division of cartilage tissue (chondrocytes), while the production of pro -inflammatory cytokines is increased, which is usually present in cartilage in only small quantities.The cytokines launch the inflammatory process, for example, under the influence of pro-inflammatory cytokine IL-1, enzymes are separated that destroy the collapse of the joint.Under the influence of cytokines, the production of the TSOG-2 enzyme and other substances that have a toxic effect on cartilage.
Synovites also play a major role in the development of coxarthrosis - inflammatory diseases of the synovial shell of joints or ligaments with accumulation of fluid in the cavity.
A decrease in the elasticity and strength of the articular cartilage associated with the metabolic disorders leads to a decrease in its resistance to mechanical stress.With cox arthrosis, all components of the joints are involved in the pathological process, including a subchondral bone.Due to the fact that large collections of the lower extremities account for large joints in the body, they experience considerable mechanical stress due to which microvalomas occur in the subchondral plate and cartilage.As a result of micro -nomes, the subchondral bone is compressed, leading to the regional growth of bone tissue - osteophytes.And this stimulates further degradation of the articular cartilage.
In some cases, arthrosis of the hip joint is inherited.Hereditary arthrosis is reportedly polygen inheritance - due to the effect of many genes, each of which affects weak.The cause of some diseases is a mutation in genes that encode macromolecules of articular cartilage, causing its fracture.Genes responsible for the division of chondrocytes also like.In addition, metabolic disorders are inherited, such as pyrophosphate arthropods - a disease in which crystals of calcium pyrophosphate accumulate in the articular cartilage and synovial fluid.
Classification and phases of development of arthrosis of the hip joints
Depending on the causes of the disease, coxarthrosis is divided into two main forms: primary (idiopathic) and secondary (that occurs from or due to other diseases).
Primary Cox arthrosis:
- Located (hip joints only affect):
- unilateral;
- Bilateral.
- Generalized (polyosteoarthrosis) with a lesion of at least three joints (for example, hip, knees and small joints of brushes or feet).
Secondary Arthrosis:
- Post -Traumatic:
- Acute - as a consequence of acute injury;
- Chronic - due to classes of some sports or as a result of professional activity.
- Metabolic diseases (oconosis, hemochromatosis, wilson's disease, gaucher disease).
- Congenital pathologies and developmental defects (congenital dysplasia of the hip joint, perte disease, slip of the epiphys of the femur, hypermobility syndrome, abbreviation of the lower extremity, scoliosis, bone displasia).
- Endocrine pathologies (acromegaly, hypothyroidism, diabetes mellitus, hyperparathyroidism, obesity).
- Calcium salts (pyrophosphate arthropod, calcification of tendon inflammation).
- Diseases with bones and joints (rheumatoid arthritis, psoriasis arthritis, petic disease, avascular necrosis, infections).
According to clinical manifestations, the following forms of coxarthrosis are separated:
- Small symptomical.
- Manifesto, manifested by bright clinical symptoms:
- rapidly progressively, where symptoms develop in the first four years from the beginning of the disease;
- Slow progressive - clinically significant symptoms appear after five years after the illness.
In accordance with the X -Ray image, two types of arthosis of the hip joints can be identified:
- Hypertrophic - with signs of increased repair response (lesions are replaced by a new tissue, for example osteophytes);
- Atrophic (decrease in tissue volume).
The stages of the disease can be determined radiologically and clinically.To determine the radiological phase of arthrosis of the hip joint, the classification of Kellgren and Lawrence (1957) is most often used.
Phases of Arthosis in Radiological Classification
| Phase | Sign |
|---|---|
| 0 | There are no signs of arthrosis in x -Ray images |
| 1 | The common gap does not change, single regional osteophytes visualized |
| 2 | The common gap does not change, significant regional osteophytes visualized |
| 3 | The height of the common gap is moderately reduced, significant regional osteophytes visualized |
| 4 | The height of the common gorge is significantly reduced, significant regional osteophytes and subchondral osteosclerosis visualized (bone tissue under the lower surface of cartilage with the cartilage structure) |
To determine the clinical phase of the disease, classification (1961) is used, which uses both clinical signs and visualization criteria.
Clinical stages of arthrosis
| Phase | Sign |
|---|---|
| 0 | The articular gorge is narrowed unequivocally and unevenly, the edges of the articular cracks are a little pointed (initial osteot huts), a slight limitation of movements noted |
| 1 | The articular gorge is significantly narrowed (50-60 %), significant osteophytes, subchondral osteocosclerosis and cystic information in bone piphyses;The clinic is dominated by the restriction of mobility in the joints, a rough crunch during movements, insignificant or moderate muscle atrophy |
| 2 | deformation, stiffness of the joint;The articular hole is narrowed by more than 60-70 % of the norm or completely absent, comprehensive osteophytes, subchondrial cysts, articular "mice" are visualized bones, cartilage or mixed pathological formations located in the joint cavity |
Complications of arthosis of the hip joints
With coxarthrosis, all complications are precisely associated with pathological changes in the joints.
The course of cox arthrosis can be complicated by local inflammatory processes:
- Bursite - inflammation of synovial bags in the joints;
- Tendovaginitis - inflammation of the inner shell of the vagina of muscle;
- Tunnel syndrome pinches of the nerve due to the formation of large osteophytes or with joint deformation.
With the development of coxarthrosis and its transition to II and III clinical stages, the pain limits the mobility of the joint, and over time the joint ankylosis (fibrous, bones or cartilage) accompanied by its complete immobility.
Significant joint formation can lead toFractures or aseptic necrosis of bones.For cox arthrosis, aseptic necrosis in the femoral head is the most formidable complication.
With pronounced cox arthrosis may occursubluxation and dislocation of the jointas well as the penetration of the femoral head into the pelvic cavity.Dislocations and subluxation of the hip joint leads to pain (first acute, then dull and sore), intensifies during walk and other physical exertion, as well as to deformation of the joint, limp and sometimes to shorten the affected limb.
Despite the lack of systemic manifestations of osteoarthritis itself in modern clinical practice, more attention is paid to the diseases associated with it.These are such pathological conditions that exist or occur on the basis of the current disease.In connection with inflammatory reactions that occur during arthosis, the formation of atherosclerotic plaques is improved on the inner walls of the vessels, which increases the riskCardiovascular Diseases.A decrease in physical activity due to pain and restriction of joint mobility leads toObesity, depression and deterioration of the quality of life.With prolonged use of non -steroidal anti -inflammatory drugs,The top gastrointestinal sections are affected,And tooThe risk of cardiovascular pathologies and kidney disease increases.
Diagnosis of arthrosis of the hip joints
The diagnosis of "cocoin arthritis" is made on the basis of clinical manifestations and radiological examination.There are no distinctive laboratory signs for diagnosis of arthrosis.
Among the clinical manifestationsThe head for diagnosis of arthrosis of the hip joint is the pain and its character.Pain for osteoarthritis of the hip joint occurs and gradually grows over several years (sometimes several months with a rapid progressive form).The pain occurs or improves during physical exertion or in a standing position.If the patient begins to feel pain alone, inflammation (synovitis) ended.Declaration is noticed up to 30 minutes in the morning and with prolonged immobility.
The restriction of joint mobility is gradually increased, this applies to both active and passive movements.With the development of the disease, LED can be deformed, functional abbreviation of the mud length may occur.
On a physical examinationThere is a limitation of common mobility, their deformation, abbreviation of the limbs, pain in palpation of the joint and a large spin of the femur, muscle atrophy.
Laboratory methodsFor diagnosis of arthrosis of the hip joints is not required.However, they can be used for the differential diagnosis of coxarthrosis with arthritis (rheumatoid and chronic), as arthrosis has no inflammatory changes in the total blood test and rheumatoid factor and the uric acid level is not increased.Using laboratory studies, contraindications are also revealed to drug treatment methods.
Instrumental methodsFor diagnosis of arthrosis of the hip joints:
- Radiography- This is the most important method of diagnosing arthrosis of the hip joints.The radiographer determines the changes characteristic of cocoin arthritis: narrowing the joint, osteophyt, erosion and ulceration of cartilage, subcondrial cysts and osteosclerosis.X -Ray study is a classic method of diagnosis of coxarthrosis, and radiological signs underlie the classification of coxarthrosis.At present, however, other methods of visualization of the joint are increasingly used, such as ultrasound and magnetic resonance image.
- Ultrasound examination (ultrasound) -The advantage of ultrasound is in the absence of a radial strain on the body.
- Magnetic Resonance Tomography (MRI)- In comparison with other methods, it allows you to more clearly visualize joint damage.
- ArthroscopyAndAllows you to identify damage to the articular cartilage: from zones of chondomation (softening of the articular cartilage) with a diameter of less than 10 mm to deep cracks that penetrate the subcondrial bone and the formation of deep stomach ulcers.Superficial and medium -sized cracks and erosion of surfaces can also be visualized.
The identification of cox arthrosis does not usually represent special difficulties, but when assessing a specific clinical situation, it is necessary to remember the possible secondary origin of arthrosis of the hip joints (such as complications of other diseases, for example with endocrine suffering).
Treatment of arthrosis of the hip joints
Treatment of arthrosis of the hip joints can be both conservative (medicine and not -assembled) or operational.Conservative treatment is used in 1-2 stages of the disease, surgical-in 3 stages.Surgical treatment can be recommended at 2 stages with persistent pain and lack of reaction to conservative therapy.
The goals of conservative therapy:
- Improve the quality of life - reduce pain and increase the common mobility;
- Stop or slow down the development of the disease.
Non -Eve treatment methods include:
- Reading the hip joint (decrease in body weight, creating additional support and transfer of part of the body weight to sugar cane or crutches);
- Physiotherapy Physical Education;
- Physiotherapeutic treatment methods.
Treatment of coxarthrosis begins with non -Drug methods, which is given an important role in physical therapy exercises.With severe pain, the patient should use the support.With a pronounced disease and the presence of contraindications to endoprotetics, support must be used for life.
Medical therapy of cuxarthrosisIncludes drugs that reduce the symptoms of the disease.These are painkillers as well as drugs from the group of non -steroidal anti -inflammatory drugs (NSAIDs).The NSAIDs are divided into non -selection and selective.
Analgesics and NSAIDs for arthrosis of the hip joint are used for a short time to relieve pain and inflammation.Currently, there is no documented advantage of a non -steroid anti -inflammatory agent above another, so the choice of one particular drug depends on the side effects and a specific clinical situation caused by it.
It should be remembered that NSAIDs have a number of side effects.When taking them, the mucosa of the stomach and duodenum is affected, as a result of gastric ulcer and bleeding possible.A number of NSAIDs have a toxic effect on the liver and kidneys.In addition, NSAIDs disrupt the platelet aggregation and, as a result, the patient is disturbed by thrombosis and there is a tendency for bleeding.The NSAIDs with prolonged use suppress the processes of hematopoiesis and can cause aplastic anemia and agranulocytosis.Receiving Selective NSAIDs causes significantly less complications.
Ointments and gels used locally cause minor side effects than oral products.For the treatment of arthrosis, drugs are used with heating and reduction of pain.They can contain terpentine, menthol, nicotic acid testers, salicylates, bee poison.The NSAIDs also have a good effect.
In the absence of the effect of painkillers and NSAIDs, or if it is impossible to choose the optimal dose of the drug, painkillers in central action can be prescribed briefly.
In case of inflammation, intra -articular submission of corticosteroids is used.Corticosteroids are used no more than 2-3 times a year, as more frequent use can lead to cartilage degeneration.
Slow -acting drugs weaken the symptoms of the disease include chondroprotectors, inappropriate compounds of avocado or soy, hyaluronic acid.These medicines are included in the recommendations of the European Antirematic League for the treatment of arthrosis of the hip joints.Preparations reduce pain and improve joint mobility.
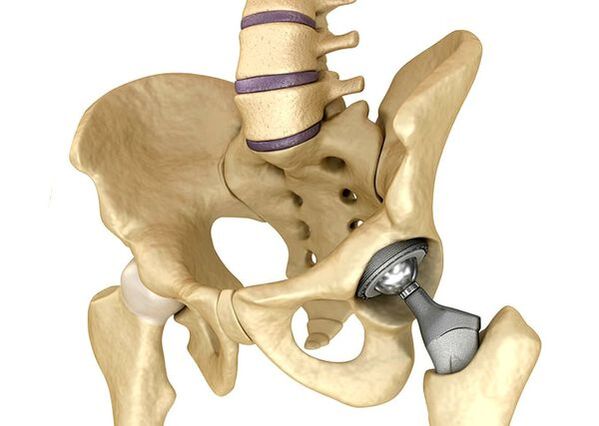
Endoprotetics of the hip jointsIt is used in severe cases of phase III when the pain syndrome cannot be removed and the mobility of the collection is significantly limited.Protetics of the hip joint leads to a decrease in the pain syndrome, an improvement in the functional condition of the joint and the quality of the patient's life.The effect persists for 10-15 years, after which another operation may be required.During the operation, the hip joint is replaced by artificial imitation of ceramics, metal (most commonly used titanium prostheses) or polymer.
Forecast.Prevention
The prognosis of arthrosis of the hip joints in relation to the patient's life is favorable, but the disease often leads to disability.According to the World Health Organization, 80 % of elderly patients with coxarthrosis have a violation of mobility and 25 % cannot make everyday conditions.In this regard, the primary prevention of arthrosis of the hip joints is important.
Prevention Measures:

- Reduce body weight.It is necessary to adjust nutrition to reduce the weight and load on the joint.In addition, a decrease in the volume of adipose tissue reduces the amount of inflammation intermediaries it released.
- Avoid heavy physical work and sports overload.Physical overloads are often the cause of arthrosis of the hip joints, while moderate physical activity, on the contrary, improves the condition of the articular cartilage, retains its normal mobility and reduces the load on other joints.
- Correcting the underlying disease.If the patient is detected in diseases that can lead to secondary cocoin arthrosis (endocrine, rheumatic and others), the underlying disease is necessary.The normalization of the hormonal background and the achievement of sustained remission of rheumatic diseases is both the primary prevention of arthrosis and allows you to slow its development.
- Lead a healthy lifestyle.A balanced diet with a sufficient content of plant and animal protein, polyunsaturated fatty acids and limitation of simple carbohydrates as well as moderate physical activity avoids the occurrence of coxarthrosis, even in the presence of risk factors.
Currently, the prevention of diseases of the hip joint is mandatory in neonatology and pediatrics.Over time, the adjusted congenital dysplasia of the hip joint significantly reduces the risk of coxarthrosis in adult age.